

MD Psychiatry Resident, MBBS
Share this story
You eat something perfectly healthy — a bowl of lentil soup, a banana, a handful of almonds — and within the hour, you're bloated enough to look three months pregnant. You're not imagining it, and it's not random.
If you have SIBO, the bacteria overgrown in your small intestine are fermenting that food before your body absorbs it. They produce gas, cause inflammation, and make eating feel like a game you can't win. The cruel irony is that many of the foods driving this are ones most people would call clean or nutritious.
The right diet won't cure SIBO on its own, but it's a critical part of the recovery process. It reduces symptoms while treatment clears the overgrowth, and it helps prevent the bacteria from coming back once you do.
What is SIBO?
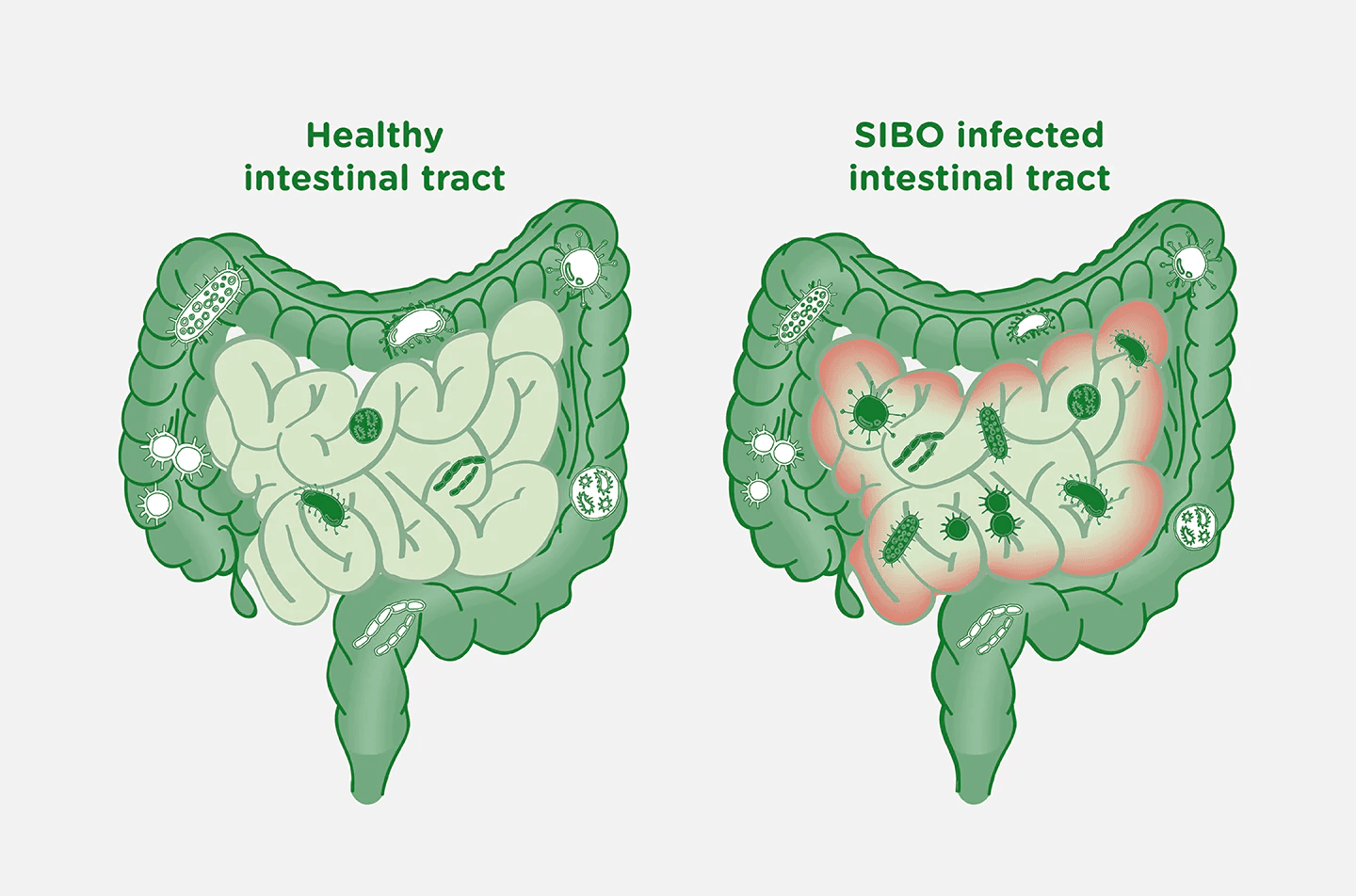
SIBO stands for small intestinal bacterial overgrowth. Under normal conditions, your small intestine has a relatively low bacterial count, fewer than 1,000 colony-forming units per milliliter. In SIBO, bacteria colonize this space in excess, ferment the food passing through, and produce gases that the small intestine has no good way to expel.
Symptoms include bloating, gas, abdominal pain, diarrhea, constipation, and in more severe cases, nutritional deficiencies. Because the small intestine is where most absorption happens, an overgrowth there can interfere with your ability to absorb iron, vitamin B12, and fat-soluble vitamins like D and K.
The type of gas the bacteria produce matters. Hydrogen-dominant SIBO tends to cause diarrhea, while methane-dominant overgrowth is more associated with constipation. Hydrogen-sulfide SIBO often causes a distinctly foul-smelling gas. Knowing your subtype helps determine which dietary approach fits best.
Why your food choices matter so much with SIBO
The simple version: bacteria in the small intestine feed primarily on carbohydrates. When you eat fermentable carbohydrates — sugars, certain starches, and fibers that the small intestine can't fully absorb — those carbohydrates sit in the small intestine long enough for bacteria to ferment them. The bacteria multiply and produce more gas. Symptoms follow.
Fats and proteins behave very differently. They're absorbed efficiently in the upper small intestine, leaving almost nothing for bacteria to work with. This is why someone with SIBO can usually handle a plate of salmon, roasted zucchini, and white rice without issue, but struggles badly after a bowl of chickpea curry or a glass of regular milk.
According to Cleveland Clinic gastroenterologists, every proposed SIBO dietary approach is built on this same principle: limiting fermentable carbohydrates to starve the overgrowth. The diets differ in how restrictive they are, not in their core logic.
Diet alone won't eliminate SIBO. You'll likely need antibiotics like rifaximin, herbal antimicrobials, or an elemental diet protocol. But eating the wrong foods during treatment keeps fueling the bacteria you're trying to clear. And eating strategically after treatment lowers your relapse risk considerably.
The low-FODMAP diet: the most evidence-backed starting point
The low-FODMAP diet is the most widely studied dietary approach for SIBO and the closely related condition IBS. (If you already manage IBS alongside your SIBO, the foods that trigger IBS flares overlap significantly with the SIBO trigger list below.) FODMAP stands for fermentable oligosaccharides, disaccharides, monosaccharides, and polyols. These are four groups of carbohydrates that the small intestine absorbs poorly and bacteria ferment rapidly.
A 2024 umbrella review analyzing 16 meta-analyses covering over 9,900 patients found that a low-FODMAP diet significantly reduced symptom severity and improved quality of life in people with IBS. While studies specifically targeting SIBO populations are smaller, SIBO and IBS overlap so frequently that clinicians routinely apply low-FODMAP principles to both.
Research also indicates that 60 to 70% of IBS sufferers experience meaningful symptom relief on this plan. Given the symptom overlap with SIBO, this is a meaningful starting benchmark.
The diet runs in three phases: elimination, reintroduction, and personalized maintenance. The elimination phase typically lasts four to six weeks. It's restrictive by design and not intended as a permanent way of eating.
Foods to eat with SIBO
These are the foods most people with SIBO tolerate well. They're low in fermentable carbohydrates, which means bacteria in the small intestine have very little to work with.
Proteins (unrestricted)
All animal proteins are safe. Chicken, turkey, beef, pork, fish, seafood, and eggs are absorbed almost entirely in the small intestine, leaving little residue for bacteria to ferment. When I'm supporting clients through a rough patch of gut symptoms, eggs and grilled fish are always the most reliable anchors because they're consistently well-tolerated regardless of what else is going on.
Fats (unrestricted)
Olive oil, butter, ghee, and coconut oil are all safe. Avocado is technically a fruit but belongs here in practical terms. According to Monash University's FODMAP testing, a serving of about one-third of a medium avocado is low-FODMAP and well-tolerated by most people with SIBO.
Low-FODMAP vegetables
Carrots, zucchini, bell peppers, cucumber, eggplant, green beans, bok choy, lettuce, kale, and tomatoes are all in the safe column. These are low in fructans and polyols, the two FODMAP groups most reliably associated with SIBO symptoms.
Low-FODMAP fruits
Strawberries, blueberries, raspberries, oranges, grapes, and small portions of unripe banana are generally well-tolerated. Ripe bananas and most stone fruits (peaches, plums, nectarines) are higher in sorbitol and are better avoided in the elimination phase.
Grains and starches
White rice is the safest grain for SIBO. Small portions of oats, quinoa, and gluten-free bread made from rice or corn flour are also options, though individual responses vary. Long-fermented sourdough bread is lower in fructans than regular wheat bread, because the fermentation process breaks down a significant portion of the oligosaccharides.
Lactose-free dairy
Regular dairy contains lactose, a disaccharide FODMAP. Lactose-free milk, hard aged cheeses (cheddar, parmesan, brie), and lactose-free yogurt are good substitutes. Butter contains negligible lactose and is fine.

Foods to avoid with SIBO
During the elimination phase, these foods give bacteria the fermentable fuel they need most. Remove them for four to six weeks.
High-fructan foods (the biggest offenders)
Garlic and onions sit at the top of almost every SIBO trigger list for good reason. They're extremely high in fructans, the oligosaccharide that gut bacteria ferment fastest. Even small amounts of garlic can trigger significant symptoms in people with active SIBO. Other high-fructan foods to remove include wheat, rye, barley, asparagus, leeks, shallots, and artichokes.
Legumes
Lentils, chickpeas, kidney beans, black beans, and most other legumes are high in galacto-oligosaccharides, another FODMAP group that bacteria ferment aggressively. Canned and rinsed legumes have lower oligosaccharide content than dry-cooked, but they're still best avoided in the elimination phase.
High-lactose dairy
Regular cow's milk, soft cheeses like ricotta and cottage cheese, yogurt made with regular milk, and cream-based dishes are all high in lactose. Eliminate these in phase one and test them systematically during reintroduction.
High-fructose foods
Honey, high-fructose corn syrup, mango, ripe pears, watermelon, and apples are high in fructose. Fructose is poorly absorbed in the small intestine of many people, and in someone with SIBO, it becomes quick fermentation fuel.
Sugar alcohols (polyols)
Sorbitol, mannitol, xylitol, and erythritol — found in sugar-free gum, mints, and most "low-sugar" products — are highly fermentable and among the most reliable symptom triggers in SIBO. Check ingredient labels carefully. Many protein bars and low-carb snacks contain these without being obvious about it on the front panel.
Large portions of cruciferous vegetables
Broccoli, cauliflower, Brussels sprouts, and cabbage contain both fructans and sulfur compounds. Small portions (about 75g of broccoli) fall within the low-FODMAP threshold according to Monash testing, but larger portions push into high-FODMAP territory quickly. People with hydrogen-sulfide dominant SIBO may need to reduce sulfur-rich foods more broadly, at least temporarily.
The three phases of a SIBO diet
The SIBO diet is a process, not a permanent food list. Moving through the phases properly is what makes the difference between short-term symptom relief and lasting recovery.
Phase 1: Elimination (weeks 1 to 6)
Remove all high-FODMAP foods. Stick to the safe foods in the list above. This phase works best when combined with your actual SIBO treatment, whether that's rifaximin, herbal antimicrobials, or an elemental protocol. The diet reduces the bacteria's food supply; the treatment reduces the bacteria themselves.
Don't extend this phase unnecessarily. Prolonged elimination without reintroduction can reduce gut microbial diversity over time and make the reintroduction phase harder.
Phase 2: Reintroduction (starting around week 6)
Reintroduction is the phase most people skip, and that's a genuine mistake. Without it, you end up unnecessarily restricting foods for years that you probably tolerate fine.
Introduce foods one at a time, in small portions, over three-day intervals. If a food causes no symptoms over those three days, it's likely safe for you to keep eating. If it causes symptoms, remove it and try again once your gut has settled further. A food diary is useful here.
The goal is the least restrictive diet that keeps you symptom-free, not the elimination protocol extended indefinitely.
Phase 3: Long-term maintenance
Once you know your specific triggers, your diet becomes personalized rather than protocol-based. Most people find they can reintegrate a wide range of foods after successful SIBO treatment.
The most important thing in this phase is addressing the underlying cause of your SIBO. Slow gut motility, low stomach acid, anatomical changes from surgery, or long-term PPI use can all allow bacteria to re-establish themselves in the small intestine. Without treating the root cause, dietary management alone will reduce symptoms but won't prevent recurrence.
Other dietary approaches worth knowing
Low-FODMAP is the most evidence-backed starting point, but it's not the only option.
The elemental diet
The most aggressive dietary intervention for SIBO. An elemental diet consists of pre-digested nutrient shakes, with amino acids, simple sugars, and fats that absorb in the upper small intestine and leave nothing for bacteria to ferment. A 2025 prospective study published in Clinical Gastroenterology and Hepatology found that after two weeks of exclusive elemental diet, 73% of participants showed breath test normalization and 83% reported meaningful symptom improvement. It works, but two weeks of nothing but shakes is demanding. It's typically used for people who haven't responded to antibiotics or standard dietary interventions.
The Specific Carbohydrate Diet (SCD)
The SCD eliminates all grains, lactose, and refined sugars, and focuses on monosaccharide carbohydrates that are easily absorbed. Most research on the SCD is in Crohn's disease rather than SIBO specifically. It's more restrictive than low-FODMAP, harder to sustain, and clinicians generally recommend starting with low-FODMAP first before considering the SCD.
The low-fermentation diet
Developed by SIBO researcher Dr. Mark Pimentel at Cedars-Sinai Medical Center, this approach focuses on limiting carbohydrates that aren't fully digested in the small intestine. It places additional emphasis on meal timing, specifically leaving longer gaps between meals to allow the migrating motor complex (the gut's self-cleaning mechanism) to sweep bacteria toward the colon. There's significant overlap with low-FODMAP, and it's gaining attention as a SIBO-specific framework.
Final thoughts
The core logic of the SIBO diet is simple: remove the food supply for the bacteria, and you reduce one of the biggest drivers of your symptoms. The low-FODMAP diet is the strongest evidence-backed starting point. It's flexible enough to stay nutritious, and when combined with proper medical treatment, it gives your gut a real chance to recover.
The diet alone isn't enough. If you've been living with recurring bloating, gas, and unpredictable digestion, work with a gastroenterologist or registered dietitian who understands SIBO, especially for the reintroduction phase. That's where most people stall, and where professional guidance makes the biggest difference in long-term outcomes.
For a deeper look at how gut bacteria affect your mood, focus, and stress response far beyond digestion, the gut-brain connection post is a useful next read.
Got questions? Ping me on LinkedIn.





