
طبيبة مقيمة في الطب النفسي، MD، MBBS
شارك هذه القصة
Introduction
If you have PCOD—Polycystic Ovarian Disease—you've probably heard conflicting advice: cut carbs, eat keto, take supplements, track calories obsessively. Some of it contradicts itself. Some of it works for two weeks. Most of it makes you feel worse.
Here's the thing nobody tells you plainly: PCOD is not a weight problem. It's a hormonal problem that manifests as a weight problem. And that distinction changes everything about how you should eat.
For the last three years, I've worked with women managing PCOD, seen what actually moves the needle on their labs, and watched how the right nutritional framework—not the trendiest one—creates sustainable recovery. This guide covers the science behind why your body behaves the way it does, and exactly how to eat to work with your physiology instead of against it.
What PCOD Actually Is (And Why Your Diet Matters)
PCOD is a hormonal condition where your ovaries produce eggs that either don't mature fully or mature and turn into small cysts. This doesn't always mean irregular periods—PCOD is more subtle than that. But it does mean your hormones are dysregulated.
The root cause? In 70–80% of cases: insulin resistance.
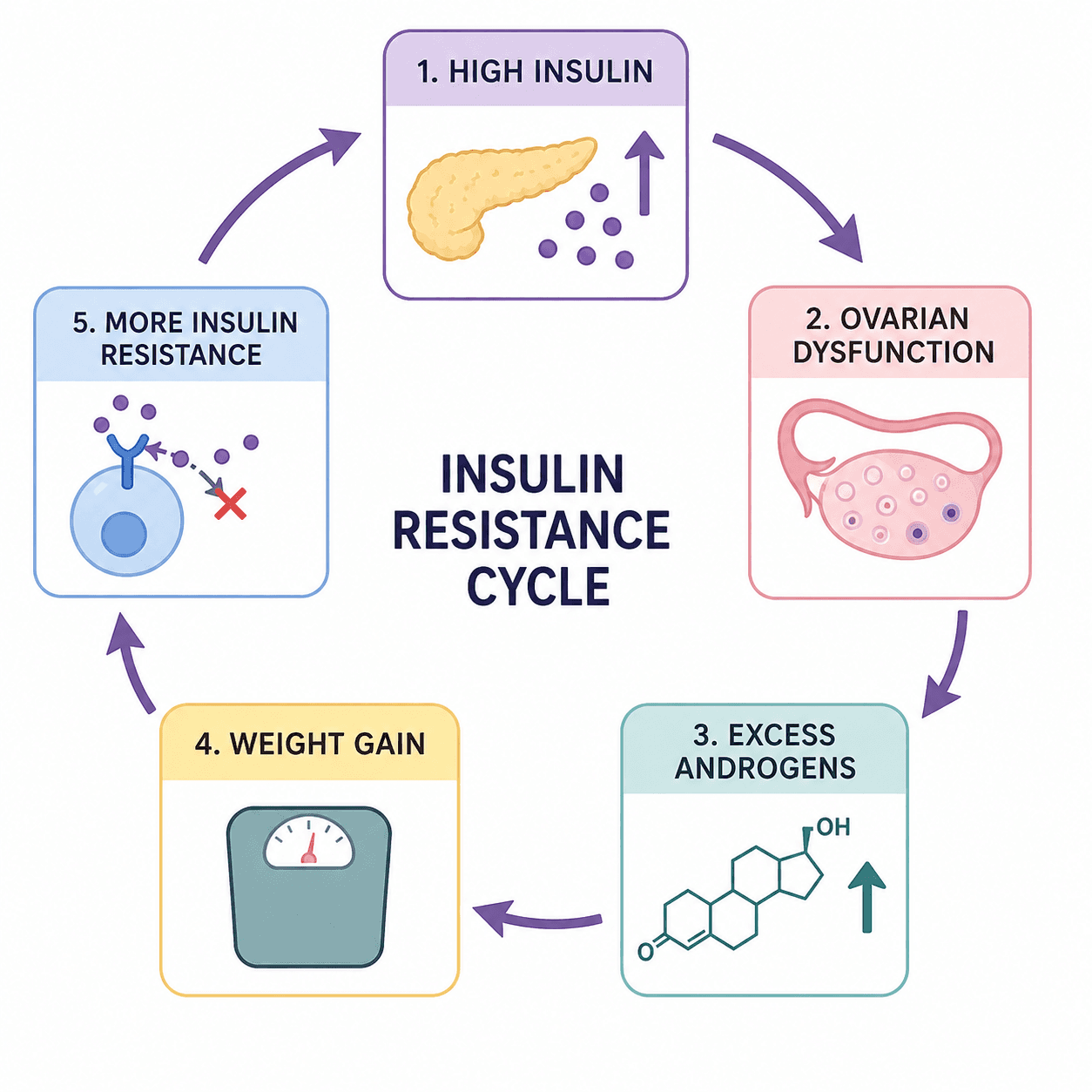
Your cells stop responding efficiently to insulin, so your pancreas pumps out more and more to get the job done. That excess circulating insulin travels to your ovaries and tells them to make androgens (male hormones). Extra androgens mess with your menstrual cycle, trigger acne and hair loss, and make fat loss feel impossible. Meanwhile, that constant high insulin levels also worsen inflammation throughout your body—the low-grade, systemic kind that accelerates aging and increases disease risk.
The cruel irony: excess insulin makes your body store fat more aggressively, especially around your midsection, which then worsens insulin resistance. You're trapped in a vicious cycle.
Diet is the primary lever you have to break this cycle. Not willpower. Not exercise alone. Not supplements. Diet.
The Three Core Pillars of a PCOD-Friendly Diet
Pillar 1: Stabilize Blood Sugar with Low Glycemic Index Carbs
Your first job is to stop triggering massive insulin spikes.
The glycemic index (GI) measures how quickly a food raises your blood sugar. High-GI foods (white bread, instant oatmeal, fruit juice) cause rapid glucose spikes, which demand rapid insulin responses. Over time, repeated spikes worsen insulin resistance.
Low-GI foods digest more slowly, releasing glucose steadily. This keeps insulin levels stable and gives your cells a fighting chance to become sensitive to insulin again.
Why this matters for PCOD: Research published in peer-reviewed journals shows that women with PCOD who switch to a low-GI diet—without even cutting calories—improve insulin sensitivity, reduce androgen levels, and restore menstrual regularity. One study found that within three months, women on a low-GI diet had significant improvements in fasting insulin and testosterone levels compared to women eating an identical number of calories on a high-GI diet.
What low-GI carbs look like:
Whole grains: Steel-cut oats, brown rice, quinoa, barley, farro, millet
Legumes: Lentils, chickpeas, black beans, kidney beans (these are also high in fiber and protein—the trifecta)
Vegetables: All non-starchy vegetables. Spinach, broccoli, cauliflower, zucchini, bell peppers, tomatoes—eat freely
Fruits with restraint: Berries (blueberries, strawberries), apples, pears, oranges, guava. Limit high-GI fruits like mangoes, ripe bananas, dates, and raisins
The key is pairing any carb with protein and fat, which slows glucose absorption further. A bowl of oatmeal alone will spike your insulin. Oatmeal with Greek yogurt, almonds, and berries? That's a stable blood sugar breakfast.
Using Zorest Macro for this: The app's AI Meal Logger breaks down the carb quality of everything you log—it tells you which foods are triggering insulin spikes and which are stabilizing your blood sugar. Over time, you build intuition for carb choices without obsessing over GI numbers.
Pillar 2: Eat Adequate Protein at Every Meal
Protein is non-negotiable for PCOD. Here's why:
It stabilizes blood sugar: Protein slows gastric emptying, which means carbs enter your bloodstream more gradually.
It preserves muscle during fat loss: Women with PCOD often lose weight, but without enough protein, they lose muscle too—which further damages metabolism.
It increases satiety: You feel fuller longer, which naturally reduces overeating.
It has a thermic effect: Your body burns ~25% of protein calories just digesting it, compared to ~10% for carbs and ~3% for fat.
How much? Aim for 1.2–1.6g of protein per kilogram of body weight daily. If you weigh 70kg, that's roughly 85–110g per day. Spread it across meals—not all at dinner.
Best protein sources for PCOD:
Fish (salmon, mackerel, sardines): High in omega-3 fatty acids, which are anti-inflammatory. Eat 2–3 times per week
Eggs: Whole eggs, not just whites. Choline in egg yolks supports hormone metabolism
Poultry: Skinless chicken and turkey, lower in saturated fat
Legumes: Lentils, chickpeas, black beans. They're protein and fiber—a nutrient density power play
Paneer and Greek yogurt: Good protein-to-calorie ratio; low-fat versions work well
Tofu and tempeh: If you eat plant-based, these are your anchors
Real example: Your breakfast isn't toast. It's whole grain toast with Greek yogurt, berries, and a drizzle of honey. Lunch isn't a salad. It's grilled salmon over mixed greens, quinoa, and olive oil dressing. Dinner isn't pasta. It's lentil pasta (yes, they exist) with chicken and lots of vegetables.
Pillar 3: Deliberately Include Anti-Inflammatory Foods
PCOD is a low-grade inflammatory condition. Your immune system is in mild overdrive, which accelerates tissue damage and worsens insulin resistance. Anti-inflammatory foods dial down this activation.
Why this works: Chronic inflammation drives the insulin resistance → hormone dysfunction cycle. By reducing inflammation through food, you reduce the underlying driver of PCOD.
Anti-inflammatory foods to prioritize:
Fatty fish: Salmon, mackerel, sardines (omega-3s reduce inflammatory markers)
Leafy greens: Spinach, kale, arugula (rich in antioxidants)
Berries: Blueberries, strawberries, raspberries (contain anthocyanins, potent anti-inflammatory compounds)
Extra virgin olive oil: Use it on salads, vegetables, or as a finishing oil. The polyphenols are anti-inflammatory
Nuts and seeds: Almonds, walnuts, chia seeds, flax seeds (contain alpha-linolenic acid, an omega-3 precursor)
Turmeric: Active compound curcumin is a proven anti-inflammatory. Add it to curries, scrambled eggs, or roasted vegetables
Ginger: Fresh or powdered; steep in tea or add to stir-fries
Garlic and onions: Contain sulfur compounds that reduce inflammation
Green tea: EGCG, a polyphenol, has documented anti-inflammatory effects. Drink 1–2 cups daily
A Mediterranean-style eating pattern—high in fish, olive oil, vegetables, legumes, and nuts—is the gold standard for PCOD. Studies show women who follow this pattern lose more visceral fat (the dangerous kind around organs) and see greater improvements in hormonal markers than women on standard low-calorie diets.
What to Eat: A Practical Food Framework
Instead of another list you'll forget, here's how to build meals:
Breakfast
Formula: Complex carb + Protein + Healthy fat + Fiber
Examples:
Steel-cut oats (complex carb) + Greek yogurt (protein) + almonds (fat) + berries (fiber)
Whole grain toast (complex carb) + 2 eggs (protein) + avocado (fat) + tomato (fiber)
Quinoa upma (complex carb + protein) + coconut oil (fat) + vegetables (fiber)
Lunch & Dinner
Formula: Lean protein + Low-GI carb + Vegetables + Healthy fat
Examples:
Grilled salmon (protein) + brown rice (carb) + roasted broccoli (vegetables) + olive oil drizzle (fat)
Lentil curry (protein + carb) + spinach (vegetables) + coconut oil (fat)
Grilled chicken (protein) + sweet potato (carb) + salad with olive oil dressing (vegetables + fat)
Snacks
Keep them protein-rich:
Greek yogurt with berries
Handful of almonds
Hummus with carrot sticks
Hard-boiled eggs
String cheese
The goal isn't perfection. It's consistency. One perfectly balanced meal doesn't fix PCOD. Fourteen days of consistently stable blood sugar does.
Foods That Actively Worsen PCOD (And Why)
High Glycemic Index Carbs
White bread, refined pasta, white rice
Instant oatmeal, sugary cereals
Fruit juices (even "natural" ones)
Baked goods, pastries, cakes
Why they're problematic: They spike insulin, which tells your ovaries to make more androgens.
Refined Sugars & Processed Foods
Candy, chocolate, desserts
Soft drinks and energy drinks
Packaged snacks (crackers, biscuits, chips)
Processed breakfast items
Why they're problematic: Double insulin hit—immediate spike, plus they're calorie-dense and nutrient-poor, so you eat more.
Inflammatory Oils & Fats
Seed oils (vegetable oil, sunflower oil, soybean oil) used in fried foods
Trans fats (partially hydrogenated oils in processed foods)
Excess saturated fat from red meat and full-fat dairy
Why they're problematic: These oils are high in omega-6 polyunsaturated fats, which promote inflammation in the body when consumed in excess (especially without offsetting omega-3 intake).
Processed & Red Meats
Bacon, sausage, deli meats
Beef and mutton (high in saturated fat and arachidonic acid, which is inflammatory)
Why they're problematic: High in saturated fat and inflammatory compounds; often contain preservatives that trigger immune activation.
Full-Fat Dairy (For Most Women)
Whole milk, full-fat yogurt, full-fat cheese, cream
Why it's complicated: Some women tolerate full-fat dairy fine; others find it worsens acne and bloating. Low-fat or fat-free Greek yogurt and curd provide the probiotic benefits without triggering symptoms.
Real talk: You don't have to eliminate these foods forever. But in the first 8–12 weeks of dietary intervention, removing them completely helps you see progress faster. Once your hormones stabilize, you can experiment with reintroducing them in moderation.
The Meal Timing Hack: Stable Eating Patterns
Here's something rarely mentioned: when you eat matters almost as much as what you eat.
Inconsistent meal timing—skipping breakfast, eating dinner at 11 PM, fasting for 16 hours then binge eating—destabilizes your entire endocrine system. Your cortisol rhythm gets disrupted, which worsens insulin resistance and increases visceral fat storage.
The science: Your cells have circadian rhythms. Eating on a consistent schedule trains your pancreas to release insulin predictably, which over weeks and months improves insulin sensitivity.
Practical framework:
Eat within 1–2 hours of waking: This stabilizes cortisol and prevents metabolic slowdown
Space meals 4–5 hours apart: Allows insulin to drop to baseline between meals
Avoid eating 2–3 hours before bed: Late-night eating disrupts sleep quality, which worsens everything
Eat at roughly the same time daily: Your body loves predictability
You don't need to count calories obsessively, but pay attention to meal size and composition. A balanced meal keeps you satisfied 4–5 hours. If you're hungry every 2 hours, your meal was carb-heavy and protein-light.
Using Zorest Macro for timing: The Daily Meal Planner generates next-day meal schedules based on your progress and your goals. It considers your typical wake time, activity patterns, and hormonal phase, so you're eating in sync with your body's needs—not fighting against them.
Hydration: The Overlooked Pillar
Most PCOD guides skip this, but dehydration actively worsens insulin resistance.
Water supports every metabolic process: glucose regulation, hormone synthesis, inflammation control, digestion, detoxification. If you're chronically dehydrated, all of these falter.
How much?: A rough baseline is 30–35 mL per kg of body weight daily. If you weigh 70kg, that's 2.1–2.5 liters. More if you exercise or live in a hot climate.
How to drink it: Not all at once. Spread it throughout the day. Small, consistent amounts are absorbed better than gulping a liter at breakfast.
What counts: Water, herbal tea, black tea, green tea. Coconut water (natural electrolytes). What doesn't count: sugary drinks, regular soda, most commercial "electrolyte" drinks (often just sugar and food coloring).
The Role of Supplements (And When You Actually Need Them)
I'm going to be direct: most supplements marketed for PCOD are overhyped and expensive.
That said, a few have evidence:
Inositol (Myo-inositol + D-chiro-inositol)
What it does: Improves insulin sensitivity at the cellular level. The evidence: Multiple randomized controlled trials show inositol supplementation improves ovulation rates, reduces androgen levels, and aids weight loss in women with PCOD. Practical dose: 2–4g daily, split across meals. Often taken as a 40:1 ratio of myo-inositol to D-chiro-inositol. Cost: Reasonable. Worth considering if your diet is solid but progress is slow.
Vitamin D
What it does: Immune regulation and insulin sensitivity. The evidence: Many women with PCOD are deficient. Correction improves ovulation and metabolic markers. Practical dose: Get your levels tested first. If deficient (<30 ng/mL), supplement 2,000–4,000 IU daily until levels normalize.
Omega-3 Fatty Acids
What it does: Reduces inflammation, improves triglyceride levels. The evidence: Particularly useful if you don't eat fatty fish 2–3 times weekly. Practical dose: 1,000–2,000 mg EPA+DHA daily.
Spearmint Tea
What it does: Anti-androgenic (reduces male hormone activity). The evidence: Two cups daily for 30 days reduces free testosterone in women with PCOD. Practical note: It's cheap. If you drink green tea anyway, swap one cup for spearmint tea.
Everything else? Skip it. Cinnamon, berberine, saw palmetto—the evidence is weak or conflicting. Your money is better spent on high-quality whole foods.
Exercise: The Synergistic Partner
Diet is 70–80% of PCOD management. Exercise is the accelerant.
You don't need to "kill it" at the gym. In fact, excessive exercise without adequate recovery worsens PCOD by elevating cortisol.
What works:
Resistance training 2–3 times weekly: 30–40 minutes. Strength training improves insulin sensitivity more effectively than cardio alone. It also preserves muscle during fat loss
Walking 30 minutes daily: Low-impact, reduces cortisol, improves cardiovascular health
One longer cardio session weekly (60 min): Running, cycling, or swimming. Shouldn't be high-intensity; should feel conversational
The synergy matters: women who combine dietary changes and exercise see 2–3x greater improvements in weight loss and hormonal markers than those who diet alone.
Real Progress Metrics (Not Just the Scale)
If you're only tracking weight, you're missing 90% of the story.
Yes, fat loss happens. But PCOD recovery shows up in ways the scale misses:
What to track:
Menstrual regularity: Are your cycles becoming more predictable? Shorter cycles (35–40 days instead of 60+) mean improving ovarian function
Skin: Reduced acne? Clearer complexion? That's falling androgen levels
Energy: Better focus, fewer afternoon crashes? That's stable blood sugar
Cravings: Are sugar cravings disappearing? That's improving insulin sensitivity
Sleep: Sleeping better? That's reduced inflammation and better cortisol rhythm
Hair: Less hair loss, slower facial hair growth? Androgens are dropping
Mood: More stable mood, less anxiety? That's hormonal equilibrium
These markers often improve before significant weight loss. If you're only watching pounds, you'll feel discouraged and quit. Track the full picture.
Labs to retest after 12 weeks:
Fasting insulin
Fasting glucose
Free and total testosterone
DHEA-S
LH/FSH ratio
Triglycerides
CRP (C-reactive protein, a marker of inflammation)
Improvement in these is the truest sign that your diet is working.
Common Mistakes (And How to Avoid Them)
Mistake 1: Crash Dieting
Eating 1,200 calories daily or less triggers metabolic adaptation. Your body senses starvation, lowers thyroid function, increases cortisol, and worsens insulin resistance. You'll lose weight initially, then plateau hard and gain it back fast.
The fix: Eat adequate calories. Use the formula: your basal metabolic rate (BMR) × 1.3–1.5. If your BMR is 1,400, eat 1,800–2,100 calories. Lose weight slowly. Sustainable is better than fast.
Mistake 2: Fasting Without Supervision
16:8 intermittent fasting, 24-hour fasts, extended fasts—they sound appealing. For PCOD, they're often counterproductive.
Extended fasting elevates cortisol and can worsen hormonal dysregulation. If you're already insulin resistant, fasting doesn't improve it—consistent, balanced meals do.
The fix: If you want to try fasting, keep it to 12–13 hours overnight. Don't fast during your luteal phase (second half of cycle) when calorie needs are higher.
Mistake 3: Obsessing Over Macros, Missing Micronutrients
You're tracking protein, carbs, and fat perfectly. But you're not eating vegetables, so you're deficient in magnesium, folate, and antioxidants. Your hormones are still dysregulated because the raw materials to make them are missing.
The fix: Protein, carbs, fats are the framework. Vegetables and whole foods are the foundation. Eat the rainbow—variety ensures micronutrient adequacy.
Mistake 4: All-or-Nothing Thinking
You have pizza on Friday, feel guilty, then eat junk all weekend because "you already failed." This cycle perpetuates dysregulation.
The fix: One meal doesn't determine your outcome. Consistency over 85–90% of your meals matters. The other 10–15%? Life happens. Move on.
Mistake 5: Ignoring Sleep and Stress
You're eating perfectly, but you're sleeping 5 hours nightly and stress-eating cortisol-driven carbs at 9 PM. Diet alone won't fix this.
Poor sleep worsens insulin resistance. Chronic stress elevates cortisol, which increases visceral fat storage and worsens androgen production.
The fix: Prioritize 7–9 hours of sleep. Manage stress—meditation, yoga, therapy, exercise. These aren't "nice to have." They're non-negotiable for hormonal recovery.
How to Start: The 30-Day Foundation Plan
You don't need perfection on day one. You need direction.
Week 1: Elimination Phase Remove the clear villains:
No sugary drinks, no candy, no pastries
No fried foods
No processed meats
No white bread, white rice, instant oatmeal
Replace with the basics:
3 meals daily, spaced 4–5 hours apart
Protein at every meal (30–40g at meals, 10–15g at snacks)
Vegetables at lunch and dinner (aim for 5–7 servings daily)
Whole grains only (brown rice, oats, quinoa, barley)
Track your energy, skin, and cravings. Many women notice improvements by day 7.
Weeks 2–4: Optimization Phase Now that you've cleared the junk, dial in anti-inflammatory foods:
Add fatty fish twice weekly (salmon, mackerel)
Use olive oil on every salad
Include a handful of nuts/seeds daily
Swap out high-GI fruits for lower-GI options (berries instead of mangoes)
Experiment with turmeric, ginger, and garlic
By week 4, you're eating in alignment with PCOD physiology. Progress happens now.
Using Zorest Macro: Log your meals for the entire 30 days. You don't have to hit perfect macros—just create consistency and visibility. The AI Coach will flag patterns: are you eating enough protein? Are your snacks stabilizing blood sugar? The app learns your patterns and adjusts its recommendations.
Beyond Diet: Lifestyle Factors That Matter
Diet is foundational, but PCOD recovery is multifactorial.
Sleep: Aim for 7–9 hours nightly, consistent bedtime. Poor sleep directly impairs insulin sensitivity.
Stress management: Chronic stress elevates cortisol, which worsens insulin resistance and increases visceral fat storage. Practice daily stress reduction: meditation (even 5 minutes), yoga, walks in nature, or therapy.
Menstrual cycle awareness: Your nutritional needs shift across your cycle. In the luteal phase (second half), your metabolic rate increases 100–300 calories. Eat more then. Track your cycle so you know when to push harder and when to rest.
Movement: Consistency beats intensity. Aim for 30 minutes of walking daily plus 2–3 resistance sessions weekly. Excessive cardio without recovery worsens PCOD.
Community: Find others managing PCOD. Isolation makes everything harder. A supportive community—online or in-person—significantly improves adherence.
The Bottom Line
PCOD is not a weight problem. It's a hormonal problem rooted in insulin resistance and chronic inflammation. Fix those two things through diet, and weight loss, regular periods, clear skin, and energy follow naturally.
The diet is straightforward:
Stabilize blood sugar with low-GI carbs
Eat adequate protein at every meal
Prioritize anti-inflammatory foods especially fatty fish, olive oil, leafy greens, and berries
Eat consistently on a stable schedule
Stay hydrated
Pair diet with movement and sleep
There's no secret supplement. No magic macro ratio. No meal plan that works for everyone. What works is understanding your body's physiology, eating in alignment with it, and being consistent for 8–12 weeks. That's when real change happens.
Progress isn't linear. Some weeks you'll feel amazing. Other weeks (especially during your cycle) you'll feel stuck. Trust the process. Your ovaries, your blood sugar, and your future self will thank you.
Medical Disclaimer
This article is educational and should not replace professional medical advice. If you suspect PCOD or have been diagnosed with PCOD, please consult a qualified gynecologist or endocrinologist before making significant dietary changes, especially if you're taking medication.


