

طبيبة مقيمة في الطب النفسي، MD، MBBS
شارك هذه القصة
Most people know vitamin K has something to do with blood clotting. Beyond that, it stays vague: one of those nutrients that shows up on food labels without earning much attention.
Here's what most nutrition content doesn't tell you: "vitamin K" is not one vitamin. It's two, and they behave very differently. One is abundant in leafy greens and easy to get. The other is mostly absent from Western diets, and its deficiency is now linked to cardiovascular disease, bone loss, and vascular calcification. You can eat plenty of spinach and still be chronically short of it.
This guide covers both forms, what they actually do, where to find them, who's at risk, and when a supplement is worth considering.
Vitamin K is actually two different vitamins
Calling vitamin K one thing is a bit like calling "omega-3" one thing. The name covers a family of fat-soluble compounds, but the two that matter for health are K1 and K2; their jobs, food sources, and deficiency risks are different enough to treat separately.
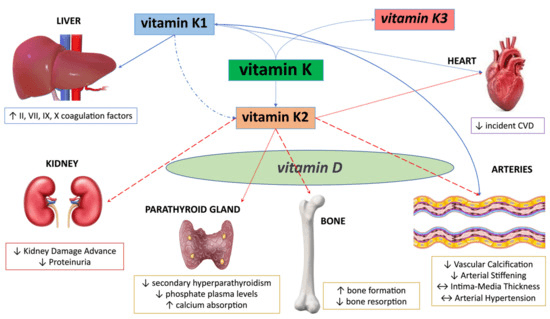
Vitamin K1 (phylloquinone) is made by plants during photosynthesis. It's found in leafy green vegetables and some vegetable oils. Once consumed, it travels primarily to the liver, where it's used to produce blood-clotting proteins. K1 makes up roughly 75–90% of all vitamin K consumed in a typical Western diet.
Vitamin K2 (menaquinones) is mostly produced by bacteria, either in fermented foods or in your gut. Unlike K1, K2 circulates in the blood for longer and reaches tissues throughout the body, including bones and blood vessel walls. This longer half-life is precisely what makes K2 so relevant to cardiovascular and bone health.
Within K2, there are subtypes. The two most studied are MK-4 (found in animal products) and MK-7 (produced by bacteria and concentrated in fermented foods like natto). MK-7 stays in the bloodstream longer and is considered more biologically active at lower doses.
What vitamin K does in your body
The classic job is blood clotting. Vitamin K activates a set of proteins called coagulation factors. Without them, even minor cuts become difficult to stop. This is the mechanism that's been known since the 1930s, when Danish researcher Henrik Dam first isolated the vitamin from chickens fed a fat-free diet.
But clotting is only the beginning.
Bone metabolism. Osteocalcin, a protein produced by bone-building cells (osteoblasts), requires vitamin K to function. Specifically, it needs to be "carboxylated," a chemical step that only happens in the presence of vitamin K, before it can bind calcium to bone tissue. Without adequate K, osteocalcin sits inactive in the bloodstream. A 2024 systematic review and meta-analysis of randomized trials found that vitamin K supplementation can help maintain or modestly improve lumbar spine bone mineral density, primarily through this carboxylation mechanism.
Vascular protection. Matrix Gla protein (MGP) is the body's main inhibitor of arterial calcification. When vitamin K is lacking, MGP stays unactivated. Calcium deposits form in artery walls instead of staying in bones. This is sometimes called the "calcium paradox": insufficient K leads to soft tissue calcification and poor bone density at the same time. Research suggests that higher K2 intake is associated with reduced risk of coronary heart disease, with one analysis finding a 9% reduction in cardiovascular mortality for every additional 10 micrograms of K2 consumed daily.
Immune and anti-inflammatory function. Emerging research shows K2 may reduce inflammatory cytokine production. Studies have found that K2 supplementation reduces C-reactive protein (CRP) levels in patients with rheumatoid arthritis. CRP is the same marker elevated in most forms of chronic systemic inflammation.
How much vitamin K you actually need
The National Academy of Sciences recommends 120 micrograms (mcg) per day for adult men and 90 mcg per day for adult women. These are Adequate Intake (AI) figures, based on the intake observed in healthy populations, not a Recommended Dietary Allowance backed by clinical trial data. The reason: there wasn't enough data to establish an Estimated Average Requirement.
Crucially, no separate recommendation exists specifically for K2. The current AI is based almost entirely on K1 intake and its effect on blood clotting. This is a gap in the nutrition science; researchers are still working to establish a K2-specific intake target. Working estimates from advocates in the field suggest 100–200 mcg of K2 per day for general health, with higher amounts potentially warranted for bone or cardiovascular concerns.
In practice, most people exceed the K1 target if they eat green vegetables. K2 is the gap, and it's a gap that often goes undetected, partly because standard blood tests don't routinely measure it.
The best food sources of K1 and K2
Getting enough K1 is relatively straightforward. Getting enough K2 requires knowing where to look.
Top K1 sources (plant-based):
Cooked turnip greens: ~530 mcg per cup
Cooked spinach: ~888 mcg per cup
Kale (raw): ~472 mcg per cup
Broccoli (cooked): ~220 mcg per cup
Brussels sprouts (cooked): ~218 mcg per cup
One serving of cooked spinach delivers more K1 than the daily AI several times over. Fat aids absorption (vitamin K is fat-soluble), so adding olive oil or butter to your greens isn't optional from a nutrition standpoint.
Top K2 sources (fermented and animal-based):
Natto (fermented soybeans): ~1,000 mcg per 100g, by far the richest source, roughly 15x more K2 than the best cheese
Jarlsberg or Gouda cheese: ~73–74 mcg per 100g
Blue cheese: ~36 mcg per 100g
Chicken (dark meat): ~35 mcg per 100g
Beef liver: ~11 mcg per 100g
Egg yolks (pastured): variable, but typically higher than factory-farmed
One caveat on animal sources: the K2 content of dairy and eggs depends heavily on what the animal ate. Grass-fed dairy and pastured eggs contain significantly more K2 than conventionally raised equivalents. The animal needs to consume K1 from grass to convert it into K2 in their tissues.
For vegans, natto is the only significant plant-based source of K2 in meaningful quantities. Sauerkraut contains some, but roughly 200 times less than natto.
Who is most at risk of vitamin K deficiency
Overt deficiency, the kind that shows up as spontaneous bleeding, is rare in healthy adults eating a varied diet. Subclinical insufficiency, particularly of K2, is considerably more common.
Groups at elevated risk include:
Newborns. Newborns are at serious risk for Vitamin K Deficiency Bleeding (VKDB) because very little K crosses the placenta, gut bacteria aren't yet established, and breast milk contains low K levels. A single vitamin K injection at birth is standard care in most countries. The proportion of newborns not receiving prophylaxis has actually increased in recent years, from roughly 3% in 2017 to over 5% by 2024, largely due to parental vaccine hesitancy extending to this intervention.
People with fat malabsorption conditions. Because K is fat-soluble, any condition that impairs fat absorption impairs K absorption. This includes Crohn's disease, celiac disease, and other gut disorders. If you're managing gut inflammation or have structural issues with your digestive tract, vitamin K status is worth reviewing with your doctor. Understanding how diet affects your gut health more broadly matters too. Our article on the SIBO diet is relevant background.
People on long-term antibiotics. Gut bacteria produce some K2. Prolonged antibiotic use disrupts that bacterial production, compounding dietary shortfalls. This is a notable issue in ICU settings, where vitamin K deficiency affects at least 20% of critically ill patients, often worsening during their stay.
Older adults. Absorption efficiency drops with age, diets become more restrictive, and the consequences of poor bone density and arterial calcification are more immediately relevant. This group also tends to take more medications that interact with vitamin K.
People on fat-blocking medications. Orlistat (the weight-loss drug sold as Alli) reduces absorption of all fat-soluble vitamins, including K. If you're using it, discuss K status with your healthcare provider.
Signs your vitamin K may be low
The classic sign is easy bruising and slow wound healing. Both reflect impaired blood clotting. Heavy menstrual bleeding in women can be another indicator.
But these symptoms only appear in frank deficiency. The subtler signs of K2 insufficiency (arterial stiffness, early-stage bone density loss, joint space narrowing) don't surface until the problem has been building for years. A 2024 Danish population-based study found elevated levels of uncarboxylated MGP (a marker of K2 insufficiency) associated with increased risk of central obesity, diabetes, and impaired kidney function. These aren't dramatic bleeding events. They're slow, silent metabolic consequences that rarely get attributed to a single nutrient.
This is why K2 status doesn't get caught in routine testing. There's no standard blood test your GP will order as part of an annual physical.

Vitamin K supplements: when they make sense
Most people can meet their K1 needs through diet. K2 is trickier, especially if you don't eat fermented foods, don't eat much animal protein, or are working against genetic variation in K1-to-K2 conversion efficiency.
When supplementing K2, the form matters. MK-7 has a longer half-life than MK-4, meaning lower doses can maintain stable blood levels. Doses studied in bone and cardiovascular research typically range from 45 to 200 mcg of MK-7 per day.
One practical point: vitamin K is often combined with vitamin D3 in supplements, and this combination makes physiological sense. Vitamin D increases calcium absorption; vitamin K2 directs that calcium to the right places (bones and teeth, not arteries). Taking high-dose D3 without adequate K2 may shift calcium toward soft tissue deposits rather than bone, a theoretical concern that has led many practitioners to recommend the two together.
The warfarin warning everyone on blood thinners should read
This section is important enough to state plainly: if you take warfarin (Coumadin) or any other vitamin K antagonist anticoagulant, vitamin K intake directly affects how your medication works.
Warfarin works by blocking vitamin K's role in clotting factor production. Changes in vitamin K intake from diet, supplements, or a new multivitamin shift the drug's effect. A sudden increase in K intake can reduce warfarin's anticoagulant effect; a decrease can intensify it.
This doesn't mean you need to avoid vitamin K entirely. In fact, maintaining a consistent vitamin K intake is generally recommended. What matters is avoiding large fluctuations. That said, any changes to diet or supplements should be discussed with your prescribing physician before you make them.
This drug interaction is also worth flagging when tracking nutrients. If you're logging your meals in Zorest Macro and you're on a blood thinner, your AI Coach can help you spot high-K days that deviate significantly from your baseline, the kind of day-to-day pattern visibility that's difficult to maintain manually.
Final thoughts
Vitamin K does more than stop bleeding. The K1/K2 distinction matters because most of us get enough of the former and not nearly enough of the latter. K2's core job is keeping calcium in bones and out of arteries, activating the proteins that govern both. That work is long-running, quiet, and visible only when it goes wrong.
If you eat green vegetables regularly, your K1 is probably fine. The real question is whether you're eating enough fermented or animal-based foods to cover K2, and whether you understand that "eating healthy" in the conventional Western sense often leaves this base uncovered.
The practical fix is specific: add natto, opt for grass-fed dairy and pastured eggs, consider an MK-7 supplement if your diet consistently misses K2 sources, and pair K2 with D3 if you're supplementing the latter at meaningful doses.
If you want a clearer picture of where you stand, log a week of honest eating. Zorest Macro's Daily Meal Planner can show you where your micronutrient gaps sit and suggest next-day meals that start closing them, including days where a single serving of dark leafy greens would push your K1 to target in under a minute of plate real estate.
Got questions? Ping me on LinkedIn.
